The Clinical Relevance of CO₂

The Clinical Relevance of CO₂
Why a colourless, odourless byproduct of metabolism sits at the very centre of everything we do under anaesthesia.
Where CO₂ comes from
Most people say the blood. Push a little further and you get to the tissues. Push further still and you reach the right answer: it all starts back at the cells.
This matters — because understanding CO₂ properly means understanding it from origin to exhaled breath. And once you do, a whole range of clinical decisions that might have seemed arbitrary start to make sense.
Every cell in the body is constantly running biochemical processes to generate energy. The primary pathway — oxidative phosphorylation — takes oxygen delivered by the blood and uses it to produce ATP, the chemical currency that powers cellular function. Carbon dioxide is a direct byproduct of this process. It is produced continuously, in every tissue, as long as the cells are alive and working.
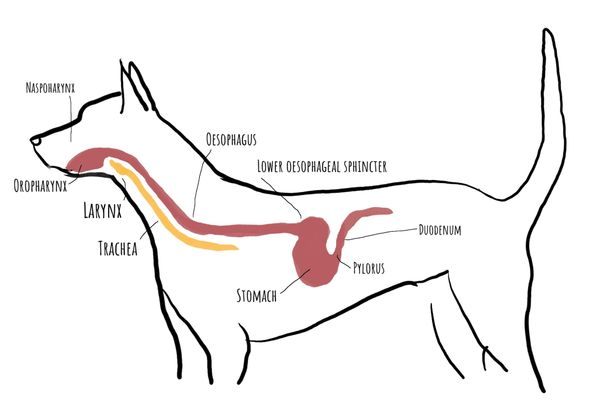
From the cells, CO₂ moves into the bloodstream. It travels in three forms: dissolved directly in plasma (a small fraction), bound to haemoglobin as carbaminohaemoglobin (a larger fraction), and — most significantly — converted to bicarbonate ions (HCO₃⁻) through a rapid enzymatic reaction in the red blood cells. This bicarbonate form accounts for around 70% of CO₂ transport and is central to understanding acid-base balance, which we will come to shortly.
The venous blood carries this CO₂ load back to the right side of the heart and then to the pulmonary circulation. In the lungs, the process reverses: CO₂ diffuses across the thin alveolar-capillary membrane, enters the alveoli, and is exhaled with each breath. This is what the capnograph measures — CO₂ at the point of exhalation, giving us a window into what is happening at the cellular level throughout the body.
- CO₂ originates at the cells — a byproduct of oxidative phosphorylation
- Transported in blood primarily as bicarbonate (HCO₃⁻ — ~70%), with smaller fractions dissolved in plasma and bound to haemoglobin
- Eliminated at the lungs by diffusion across the alveolar-capillary membrane
- The capnograph measures exhaled CO₂ — a non-invasive window into cellular metabolism and pulmonary elimination
How CO₂ is normally regulated
In a healthy, conscious animal, CO₂ is kept within a remarkably narrow range. The brainstem — specifically the central chemoreceptors in the medulla — monitors CO₂ and the associated pH in the cerebrospinal fluid continuously, and adjusts ventilation in response. This is a tight feedback loop: CO₂ rises slightly, the drive to breathe increases, more CO₂ is exhaled, levels fall back into range.
CO₂ is, in fact, the primary driver of ventilation in healthy dogs and cats. It is not oxygen that tells us to breathe — it is carbon dioxide. This is a crucial distinction, and one with important clinical consequences that we will return to at the end of this module.
The clinical experience of CO₂ accumulation is powerful and unpleasant. When CO₂ builds up and cannot be eliminated — as in a closed breathing circuit with a failing absorbent, or airway obstruction — there is a rapid and intense urge to breathe, profound distress, and a strong sympathetic response. This is the body recognising a serious physiological threat and responding accordingly. Under anaesthesia, this response is blunted — which is precisely why we need our monitors to do the job the brainstem can no longer do reliably.
- CO₂ is the primary driver of ventilation — not oxygen — in healthy dogs and cats
- Central chemoreceptors in the brainstem monitor CO₂ continuously and adjust breathing to maintain tight regulation
- CO₂ accumulation in the conscious animal produces intense distress, an overwhelming urge to breathe, and a strong sympathetic response
- Anaesthesia blunts this entire regulatory system — making monitoring essential
Why elevated CO₂ matters under anaesthesia
Under anaesthesia, several factors conspire to impair CO₂ elimination. Anaesthetic drugs reduce the sensitivity of the chemoreceptors — the CO₂ response curve shifts, so a higher CO₂ is needed to trigger the same ventilatory effort. Opioids have a particularly pronounced effect on this. Muscle relaxation reduces the mechanical effectiveness of breathing. Unusual patient positioning may limit chest wall excursion — especially relevant in obese patients, those with large abdominal masses, or patients in dorsal recumbency. And breathing circuits with narrow tubing or increased dead space raise the work of ventilation significantly.
The result can be a patient whose CO₂ climbs steadily outside the physiological range while their other parameters appear stable. So why do we care? There are three distinct reasons, and they are worth understanding separately.
Acid-base disturbance. CO₂ and pH are inseparable. When CO₂ rises, it combines with water to form carbonic acid, which dissociates to release hydrogen ions — the definition of acidosis. This respiratory acidosis matters because pH is one of the most carefully regulated variables in the body. Our drugs rely on a specific pH environment to bind plasma proteins correctly. Enzyme function is pH-dependent. Protein structure changes with pH. When pH drifts outside its narrow physiological range, many things stop working as expected — including the drugs we are relying on to keep our patient safe.
Catecholamine release. Hypercapnia triggers a sympathetic response and the release of endogenous adrenaline and noradrenaline. Under anaesthesia, this catecholamine surge has two consequences. In a patient with borderline cardiovascular function, a small bump in catecholamines may actually support blood pressure — so mild hypercapnia is not always immediately catastrophic. But in a patient who seems difficult to keep at an adequate anaesthetic depth, persistently elevated CO₂ may be contributing. The catecholamine response is actively fighting the anaesthetic, trying to wake the patient up. Regulating CO₂ removes that stimulus.
CO₂ narcosis. At very high concentrations — around 80 to 90 mmHg — CO₂ itself becomes an anaesthetic agent. It has been used in this way historically, including for the induction of anaesthesia in pigs for castration procedures. The consequence is that a patient with very severe hypercapnia may appear adequately or even deeply anaesthetised, masking a dangerous physiological state. Anaesthetic depth and CO₂ narcosis are not the same thing, and conflating them can be fatal.
- Respiratory acidosis affects drug binding, enzyme activity, and protein function — disrupting the pharmacological environment we depend on
- Catecholamine release from hypercapnia can lighten anaesthetic depth — a common but under-recognised cause of a patient that is difficult to keep anaesthetised
- Severe hypercapnia (>80–90 mmHg) produces CO₂ narcosis — CNS depression that can be mistaken for adequate anaesthetic depth
- All three effects can occur simultaneously and compound each other
CO₂ as a perfusion indicator
There is a fourth reason to monitor CO₂ that is distinct from the three above — and arguably one of the most clinically important. CO₂ is not just a ventilation monitor. It is a perfusion monitor.
Remember the pathway: CO₂ is produced at the tissues, transported in the blood, and delivered to the lungs for elimination. Every step in that chain depends on adequate circulation. If cardiac output falls — whether due to haemorrhage, myocardial depression, vasodilation, or any other cause — less blood reaches the lungs per minute. Less CO₂ is delivered to the alveoli. EtCO₂ falls.
Critically, this fall in EtCO₂ can occur despite normal or even unchanged ventilation. If your patient is being ventilated at a consistent rate and tidal volume and the EtCO₂ suddenly drops, the first question should not be about the ventilator — it should be about the circulation. A sudden, unexplained fall in EtCO₂ during anaesthesia is one of the earliest and most reliable signs of reduced cardiac output, and in the worst case, impending cardiac arrest.
This single fact transforms capnography from a ventilation monitor into a real-time indicator of cardiovascular status — and is one of the strongest arguments for considering it an essential monitor, not an optional one.
A sudden, unexplained fall in EtCO₂ during otherwise stable anaesthesia is a cardiovascular event until proven otherwise. Check perfusion — pulse quality, blood pressure, mucous membrane colour — before adjusting the ventilator.
- EtCO₂ reflects both ventilation and perfusion — blood must reach the lungs to deliver CO₂ for exhalation
- A fall in cardiac output reduces CO₂ delivery to the alveoli, causing EtCO₂ to drop even with unchanged ventilation
- Sudden unexplained falls in EtCO₂ should prompt immediate cardiovascular assessment
- EtCO₂ during CPR provides real-time feedback on compression effectiveness — a rise indicates improved pulmonary blood flow
Sources of error in CO₂ interpretation
This is a physiology module rather than a monitoring module — detailed sources of equipment error are covered in the Capnography module. But there are two interpretive errors that relate directly to the physiology we have covered here, and they are worth understanding now.
- EtCO₂ approximates but does not equal PaCO₂ — the gap widens in patients with ventilation-perfusion mismatch
- A normal EtCO₂ is reassuring in a stable patient, but always interpret it alongside cardiovascular parameters
- Never rely on a single number in isolation — CO₂ is one piece of a clinical picture
Closing pearl — the brachycephalic patient: when the rules change
Everything covered in this module assumes that CO₂ is the primary driver of ventilation — which it is, in healthy dogs and cats. But there is an important exception that every nurse working with brachycephalic patients needs to understand.
Brachycephalic dogs frequently experience chronic partial upper airway obstruction, which leads to chronically elevated CO₂ over time. The brainstem gradually adapts to this sustained hypercapnia by downregulating its sensitivity to CO₂. In the most affected individuals, CO₂ essentially loses its role as the primary ventilatory stimulus. The body switches over to using hypoxia — low oxygen — as the driver instead.
The clinical implication is significant: supplementing oxygen in these patients removes the hypoxic drive to breathe without restoring the CO₂ drive they have lost. The result can be apnoea or profound respiratory depression in a patient who appeared to be breathing adequately moments before.
Supplemental oxygen administered to a brachycephalic patient with chronic hypercapnia may remove their only remaining drive to breathe. This is not a reason to withhold oxygen when it is genuinely needed — but it is a reason to monitor closely, have assisted ventilation immediately available, and not assume that a patient breathing room air will continue to breathe normally once oxygen is supplemented.
This same phenomenon occurs in humans with obesity hypoventilation syndrome and chronic obstructive pulmonary disease — the veterinary parallel is well established. When you see a brachycephalic patient who is breathing slowly and shallowly after oxygen supplementation, do not assume they are comfortable. Check their CO₂.