Managing reflux and regurgitation during anaesthesia
Managing Gastro-oesophageal Reflux During Anaesthesia
Gastro-oesophageal reflux is one of the most consequential complications we can encounter under anaesthesia - and one of the most preventable. This module builds understanding from the ground up: what reflux is, why it happens, how to reduce the risk, and what to do when it occurs.
What happens to stomach contents when the normal barriers that keep them in place are compromised - and why does anaesthesia make this so much more dangerous?
Overview of reflux and regurgitation
When we talk about gastro-oesophageal reflux and regurgitation in the context of anaesthesia, we are talking about the movement of gastric or duodenal contents up into the oesophagus - or beyond. It is worth being precise about the terminology here, because the two terms are often used interchangeably in clinical conversation but describe subtly different processes.
Reflux is the passive movement of fluid back across the lower oesophageal sphincter into the oesophagus. It may or may not progress further. In many cases it is silent - we don't see it, we don't hear it, and the patient gives no obvious indication. This is the dangerous form, because it can cause significant harm to the oesophagus without anyone in the room realising it has occurred.
Regurgitation refers to the passive movement of gastric contents up into the pharynx or oral cavity - further along the same pathway. Unlike vomiting, regurgitation requires no active muscular effort. There is no warning, no retching, and no opportunity to intervene in the way you might with an awake patient. Under anaesthesia, with protective reflexes abolished, anything reaching the pharynx is at serious risk of entering the airway.
The two processes exist on a continuum, and understanding this matters clinically. Reflux that remains in the distal oesophagus will damage the oesophageal mucosa. Reflux that reaches the pharynx risks aspiration. Both are consequential. Neither should be dismissed.
- Reflux is the passive movement of gastric contents into the oesophagus - often silent and undetected
- Regurgitation extends to the pharynx or oral cavity, creating immediate aspiration risk
- Neither process involves active muscular effort - both are passive and unpredictable
- Anaesthesia removes the protective reflexes that would normally prevent aspiration of regurgitated material
Anatomy of the upper gastrointestinal tract
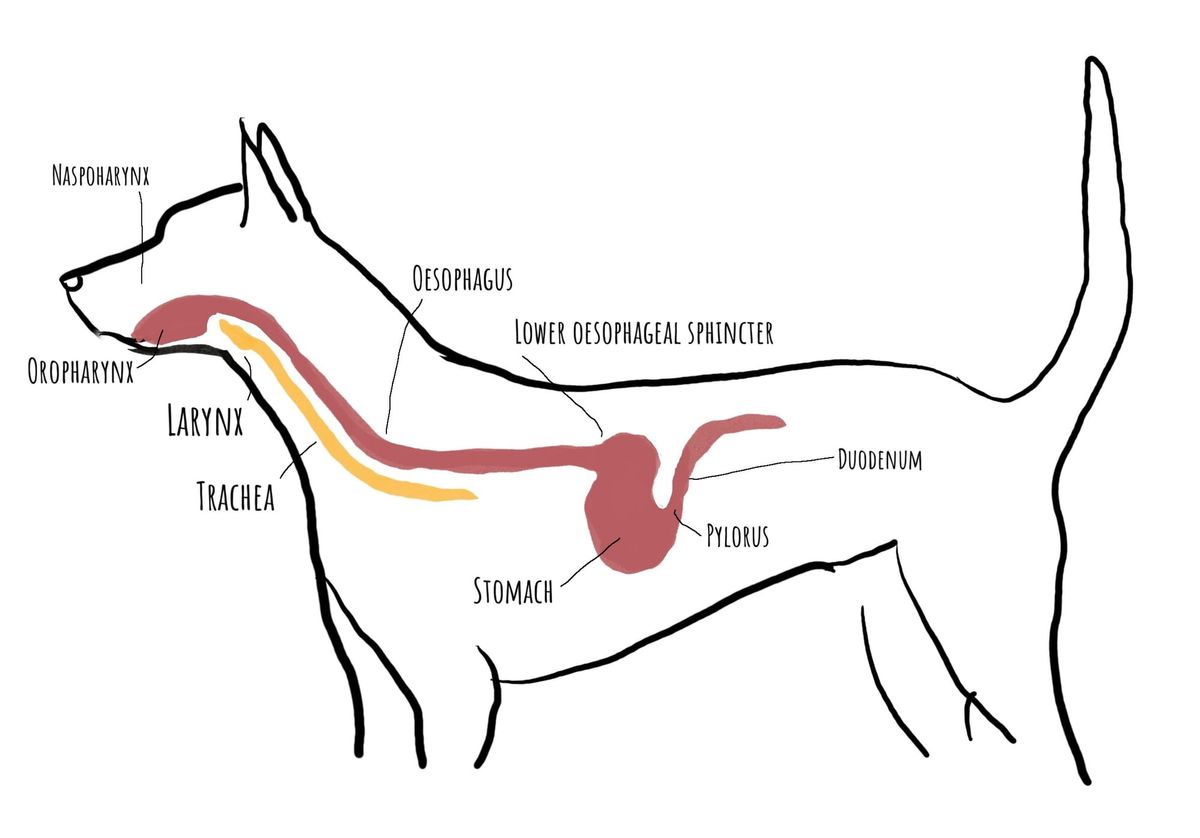
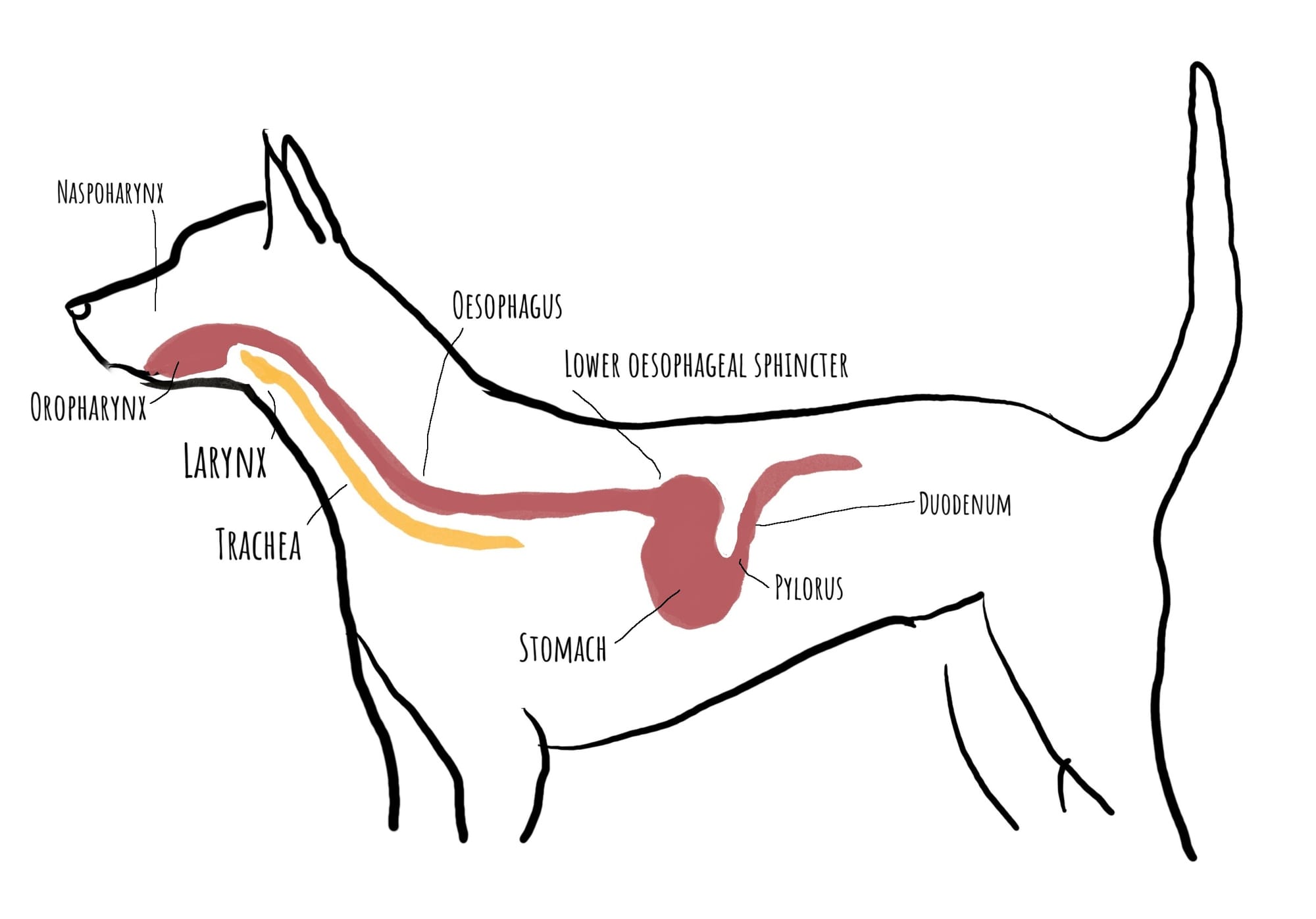
To understand why reflux is such a significant problem under anaesthesia, it helps to have a clear picture of the anatomy involved. The relevant area extends from the oral cavity all the way to the upper small intestine - and every structure along this path plays a role in either preventing or enabling reflux.
The oropharynx is the common space at the back of the mouth that connects to both the oesophagus and the larynx. In an awake animal, sophisticated reflex activity protects the larynx whenever swallowing occurs - the epiglottis closes, the vocal cords adduct, and material is directed into the oesophagus rather than the trachea. Under anaesthesia these reflexes are substantially reduced or abolished entirely.
The oesophagus runs from the pharynx through the thorax and into the abdomen, where it meets the stomach at the gastro-oesophageal junction. It is a muscular tube lined with stratified squamous epithelium - an epithelium designed for mechanical protection rather than chemical resistance. This is a critical point: the oesophageal lining is not designed to withstand the highly acidic, enzyme-rich fluid that the stomach produces.
The lower oesophageal sphincter (LOS) is the primary anatomical barrier preventing gastric contents from moving back up. It is a zone of increased smooth muscle tone at the distal oesophagus, and it is not a simple mechanical valve - its function is dynamic and influenced by a range of physiological and pharmacological factors. Many of the drugs we use in anaesthesia reduce LOS tone, making its function less reliable at exactly the moment we most need it.
Below the LOS, the stomach stores ingested material and begins the chemical and mechanical process of digestion. The pylorus regulates movement of gastric contents into the duodenum, the first part of the small intestine. Material from the duodenum - containing bile acids and pancreatic enzymes - can also reflux into the stomach and subsequently into the oesophagus. This duodenogastro-oesophageal reflux is often more chemically damaging than gastric reflux alone.
- The oropharynx is where the digestive and respiratory tracts share a common space - refluxed material reaching here is at immediate aspiration risk
- The oesophageal mucosa lacks the chemical protective mechanisms of the stomach - it is vulnerable to acid and bile injury
- The lower oesophageal sphincter is the primary reflux barrier, but its tone is dynamic and drug-sensitive
- Duodenal contents (bile acids, enzymes) can reflux into the stomach and compound the chemical injury to the oesophagus
Why is gastro-oesophageal reflux problematic?
It is worth establishing the relative frequency of these two complications at the outset. Reflux - passive movement of gastric contents into the oesophagus - is considerably more common under anaesthesia than overt regurgitation. Published data, including work by Panti et al., demonstrates that silent reflux occurs frequently, often without any clinical indication during the procedure. This matters because it shapes where we should direct most of our prevention effort: the majority of perianaesthetic morbidity from GOR comes not from aspiration pneumonia, but from oesophageal injury and subsequent oesophagitis. Aspiration, while more dramatic in its consequences, is less common - particularly when the airway is appropriately secured and any regurgitation event is recognised and managed promptly.
With that context established, the consequences of GOR fall into two distinct categories, and it is worth understanding each separately.
The first concern is oesophageal damage. The stomach produces hydrochloric acid at a pH that can fall below 2 during fasting, and the duodenum contributes bile acids and digestive enzymes. When this material contacts the oesophageal mucosa - which has no mucosal bicarbonate secretion, no mucus layer comparable to the stomach, and no acid-resistant epithelium - it causes a chemical burn. Acutely, this presents as oesophagitis: inflammation, erosion, and significant pain. You may not know it has occurred while the animal is still under anaesthesia, but you will hear about it in the days that follow as the patient shows signs of discomfort, hypersalivation, and reluctance to swallow.
The longer-term consequence of repeated or severe oesophageal injury is oesophageal stricture formation. As the damaged tissue heals, fibrous scar tissue replaces the normal mucosa, progressively narrowing the oesophageal lumen. Stricture formation is a serious and sometimes irreversible complication - affected animals may require repeated balloon dilation procedures, and some never return to fully normal swallowing function. It is a complication that is far easier to prevent than to treat.
The second and most immediately life-threatening concern is aspiration pneumonia. If refluxed material reaches the pharynx while protective airway reflexes are abolished - which is the normal state during general anaesthesia and heavy sedation - it can enter the larynx and track down into the tracheobronchial tree. Gastric fluid causes a severe chemical pneumonitis; particles of food cause mechanical obstruction and act as a culture medium for bacterial infection. The resulting aspiration pneumonia can range from a mild, self-limiting illness to a rapidly fatal condition.
What makes this particularly sobering is that aspiration under anaesthesia is often silent. The patient doesn't cough, doesn't choke, and shows no obvious sign in the moment that anything has entered the airway. The first indication may be a deterioration in oxygenation, an unexplained pyrexia in the recovery period, or a finding of pulmonary infiltrates on thoracic radiographs taken days later.
Aspiration under anaesthesia is frequently silent. There may be no coughing, no obvious distress, and no immediate clinical sign in the moment it occurs. A high index of suspicion is required in any patient known to have refluxed or regurgitated.
- Oesophageal mucosa lacks chemical resistance to gastric acid and bile - reflux causes a direct chemical burn
- Acute oesophagitis is painful and may present as hypersalivation, discomfort, and dysphagia in the recovery period
- Repeated or severe injury leads to oesophageal stricture formation - a serious, potentially irreversible complication
- Aspiration of gastric contents causes chemical pneumonitis and/or bacterial aspiration pneumonia
- Aspiration is frequently clinically silent at the time it occurs - protective airway reflexes are abolished under anaesthesia
Reasons gastro-oesophageal reflux occurs
Reflux under anaesthesia is not a single-cause problem. It arises from an interaction between patient-related vulnerabilities, the physiological effects of anaesthetic drugs, and the physical circumstances in which the anaesthetic takes place. Understanding each of these categories helps explain why some patients are at much higher risk than others - and what we can actually do to modify that risk.
The core mechanism in every case is the same: the pressure gradient across the lower oesophageal sphincter is reversed, so that gastric contents move in the wrong direction. Normally, LOS tone exceeds intragastric pressure, and material stays where it belongs. Anything that reduces LOS tone, increases intragastric pressure, or does both simultaneously moves the patient closer to that tipping point.
Patient factors
Some patients arrive with risk factors that are entirely independent of anything we do. Recognising these preoperatively is the first step toward appropriate risk stratification and planning.
Breed predisposition. Brachycephalic patients - bulldogs, pugs, French bulldogs, Boston terriers - represent a particularly high-risk population. The anatomical abnormalities that characterise brachycephalic obstructive airway syndrome generate persistently elevated negative intrathoracic pressure with every breath. Because the oesophagus runs through the thorax, this negative pressure is transmitted to it continuously. Over time and during anaesthesia, this creates a chronic tendency for gastric contents to be drawn upward across the LOS. Many brachycephalic patients also have concurrent gastrointestinal abnormalities - pyloric abnormalities, oesophageal dysmotility, and higher rates of reflux even when awake - that compound this effect.
Gastrointestinal disease. Patients with conditions that impair normal GI motility or create outflow obstruction are at significantly elevated risk. GI stasis - whether from ileus, gastric dilatation, or functional dysmotility - means the stomach contains more material for longer. Foreign body obstruction at or distal to the pylorus dramatically increases both intragastric volume and pressure. Inflammatory bowel disease, gastroenteritis, and conditions causing delayed gastric emptying all increase the amount of material available to reflux.
Obesity. Increased intra-abdominal fat raises resting intragastric pressure. Obese patients may reflux at lower thresholds than lean animals of the same species, and the increased abdominal pressure during positioning or restraint compounds this further.
Anxiety and opioid premedication. Opioid administration prior to induction substantially reduces GI motility and gastric emptying rate, effectively increasing the volume of material in the stomach at the time of induction regardless of how long the patient has been fasted.
Pregnancy. Pregnant animals carry an elevated reflux risk for several compounding reasons. The gravid uterus increases intra-abdominal pressure directly, reducing the pressure gradient across the LOS. Progesterone - elevated throughout pregnancy - has a smooth muscle relaxant effect that directly reduces LOS tone. Gastric emptying is also delayed in late pregnancy. Together, these factors make pregnant patients a high-risk group warranting the same level of precaution as a patient with GI obstruction.
Intra-abdominal masses. Any significant intra-abdominal mass - a large splenic tumour, a distended bladder, a uterine mass, or a markedly enlarged organ - increases intra-abdominal pressure and reduces the space available within the abdominal cavity. This directly raises intragastric pressure and narrows the margin between resting gastric pressure and LOS resistance. Large masses may also displace the stomach, distorting the geometry of the gastro-oesophageal junction and further compromising LOS effectiveness as a barrier.
- Brachycephalic patients carry elevated baseline risk independent of anaesthetic technique
- GI obstruction or stasis dramatically increases intragastric volume and pressure
- Obesity reduces the pressure differential that keeps gastric contents below the LOS
- Opioid premedication reduces gastric emptying - account for this when considering fasting requirements in high-risk cases
- Pregnancy raises intra-abdominal pressure, reduces LOS tone via progesterone, and delays gastric emptying - treat as high-risk
- Large intra-abdominal masses elevate intragastric pressure and may displace the gastro-oesophageal junction - assess carefully preoperatively
Anaesthetic factors
Beyond what the patient brings to the table, the drugs and techniques we choose have a direct and measurable influence on reflux risk. This is important because, unlike breed or underlying disease, these are factors we have genuine control over.
Anaesthetic depth. Both extremes of anaesthetic depth are problematic, though for different reasons. At an excessively light plane of anaesthesia, the patient retains enough muscle tone that active retching or vomiting becomes possible - particularly at induction and recovery, when depth is transitional. Gastric contents expelled with active muscular force carry higher aspiration risk than passive reflux. Conversely, an excessively deep plane prolongs the period of LOS relaxation and reduces oropharyngeal tone, keeping the pathway to the airway more patent for longer.
Opioids. As already noted in the context of premedication, opioids reduce GI motility and also directly reduce LOS tone. Morphine, fentanyl, and methadone all share this property to varying degrees. This does not mean opioids should be avoided - their contributions to balanced anaesthesia, analgesia, and reduction in inhalant requirement make them central to most anaesthetic protocols. But it is worth noting that a patient who received a morphine premedication four hours ago and then received fentanyl at induction is carrying a double hit to their LOS function throughout the procedure.
Anticholinergic drugs. Atropine and glycopyrrolate reduce LOS tone as part of their broader smooth muscle relaxant effect. This effect is clinically relevant and is one of the reasons their routine use in premedication is no longer universally recommended. Where anticholinergics are used specifically to manage bradycardia or reduce secretions, the benefit clearly outweighs the modest increase in reflux risk - but their inclusion should be a deliberate decision rather than a default.
Patient positioning and handling. Any manoeuvre that compresses the abdomen - lifting the patient by supporting the ventral abdomen, draping them over a staff member's arm, using manual pressure to restrain them - directly raises intragastric pressure. The LOS may be adequate at rest and inadequate under the increased pressure of careless handling. This risk is highest at induction and recovery, when depth is transitional and protective reflexes are reduced without being fully abolished.
- Light anaesthetic depth allows active vomiting; deep anaesthesia prolongs LOS relaxation and reduces airway protection
- Opioids reduce both GI motility and LOS tone - relevant at premedication and throughout the procedure
- Anticholinergics reduce LOS tone - use should be deliberate rather than routine
- Physical compression of the abdomen raises intragastric pressure and can overcome LOS resistance - handling technique matters
Correct patient handling
Patient handling is one of the most actionable risk factors we have, and one of the most consistently underestimated. The practical principles are straightforward but require consistent application across the whole team - from the moment premedication is given to the point the patient is walking independently in recovery.
When lifting an anaesthetised patient, support should be placed under the axial skeleton - the pelvis, spine, and thorax - distributing the patient's weight evenly along their length. The abdomen should not bear the weight of the lift. Carrying a patient draped over a forearm, or supporting them from below the mid-abdomen, compresses the abdominal cavity and directly increases intragastric pressure. Even a brief period of abdominal compression during transfer can be sufficient to overcome the LOS in a patient whose tone is already pharmacologically reduced.
Whenever possible, anaesthetised patients should be moved on trolleys or stretchers. This distributes pressure evenly across the entire body surface and eliminates the risk of incidental abdominal compression during transfer.
Avoid placing rolled towels or positioning aids under the abdomen unless clinically necessary. Trendelenburg positioning - where the head is placed lower than the body - significantly increases the hydrostatic pressure favouring movement of gastric contents toward the pharynx and should be used with particular caution in patients with known reflux risk.
It is also worth noting that preoperative fasting duration is itself a handling and preparation consideration. Prolonged fasting - beyond six to eight hours - does not confer additional protection. It reduces gastric pH further and can increase GI motility disturbance, potentially worsening the risk profile. Current evidence supports a six-hour fast for food; this is addressed in full in the fasting section below.
Support the axial skeleton when lifting - pelvis, spine, thorax. The abdomen should not bear the weight of the lift. Apply this principle consistently at every transfer, not just at induction.
- Support the pelvis, spine, and thorax during all transfers - never the mid-abdomen
- Use trolleys or stretchers to distribute weight and eliminate abdominal compression
- Avoid positioning aids that compress the abdomen unless clinically essential
- Trendelenburg positioning (head lower than the body) increases hydrostatic pressure toward the pharynx - use with caution in high-risk patients
How to prevent gastro-oesophageal reflux
Prevention is substantially more effective than management. Once reflux has occurred, the damage to the oesophagus has already happened - and once aspiration has occurred, the clinical consequences are in motion regardless of how quickly we respond. The time spent on prevention is never wasted.
A comprehensive prevention strategy addresses every modifiable risk factor: fasting status, the choice of anaesthetic agents, airway protection, pharmacological interventions to protect the oesophagus, and the physical care of the patient throughout the perioperative period.
Anaesthetic depth and induction technique
The transition through light anaesthetic depth at induction is the highest-risk moment for active vomiting or regurgitation. An induction that is too slow - whether due to insufficient drug dose, a drug-sensitive patient receiving an overly conservative amount, or a prolonged mask induction - keeps the patient in the zone of reduced but not abolished protective reflexes for too long.
The principle of a smooth, rapid induction to an adequate depth before airway instrumentation is the single most important anaesthetic technique consideration for reflux prevention. A patient that is struggling, swallowing, or showing signs of oropharyngeal stimulation during laryngoscopy is not at an adequate depth, and intubation under these conditions carries high aspiration risk.
For high-risk patients - brachycephalics, patients with GI obstruction, those with known reflux history - pre-oxygenation allows a rapid sequence-style approach where intubation follows induction as quickly as possible, minimising the unprotected interval.
Once you have confirmed the tube is in the trachea, inflate the cuff - don't delay to check depth or connect the circuit. The tube is in the airway; securing it with an inflated cuff is the immediate priority. Depth and position can be verified once the cuff is up and the airway is protected.
It should also be noted that an insufficiently light plane of anaesthesia is itself a cause of regurgitation - not just vomiting. A patient sitting at an inadequate depth throughout a procedure has elevated reflux risk for the entire anaesthetic, not only at induction. This risk appears to be particularly relevant in orthopaedic procedures, where patient movement, positioning, and the stimulation of bone work can create periods of relative lightness that are easily underestimated.
In patients with known gastric stasis or outflow obstruction where significant fluid accumulation is suspected, it may be appropriate to decompress the stomach prior to or at induction via a naso-oesophageal or orogastric tube. Gastric volume can be assessed preoperatively using point-of-care ultrasound - a distended, fluid-filled stomach on ultrasound is a meaningful risk indicator and may guide the decision to drain before proceeding.
Pre-oxygenate high-risk patients before induction. This extends the safe apnoeic interval and allows a faster, more controlled induction-to-intubation sequence without the pressure to rush due to oxygen desaturation.
Inflate the cuff immediately upon confirmation of intubation - before positioning, before circuit connection, before anything else.
Balanced anaesthesia
The concept of balanced anaesthesia is about achieving the required anaesthetic state - unconsciousness, analgesia, muscle relaxation where needed - using a combination of agents at lower individual doses rather than relying on a single agent pushed to high concentrations. From a reflux perspective, this matters because high concentrations of inhalant agents are associated with significant LOS relaxation and GI motility suppression.
By incorporating effective preoperative analgesia (including locoregional techniques where appropriate), adequate opioid analgesia, and potentially injectable agents such as ketamine or lidocaine infusions, it is possible to maintain adequate anaesthetic depth at lower inhalant concentrations. This reduces the degree of LOS relaxation and helps preserve what residual GI tone the patient has.
The practical implication is that a well-planned anaesthetic protocol - one that uses multimodal analgesia thoughtfully - is not just about patient comfort and recovery quality. It also reduces the chemical insult to the LOS that comes with deep inhalant anaesthesia.
Preoperative fasting
Appropriate preoperative fasting is one of the most basic and most frequently misunderstood elements of reflux prevention. The goal is not simply to ensure the stomach is empty - it is to reduce both the volume and the acidity of what might be available to reflux.
The current evidence-based recommendation for elective procedures in dogs and cats is a six-hour fast for food prior to anaesthesia. This allows time for gastric emptying of a standard meal while avoiding the prolonged fasting that actually increases risk. This last point deserves emphasis: extended fasting beyond six to eight hours does not reduce reflux risk further - it may actively worsen it. A stomach that has been empty for many hours produces more concentrated, lower-pH gastric acid with no food to buffer it. The volume of fluid in the stomach actually increases with prolonged fasting as gastric secretions accumulate. The animal that was fasted overnight from 10pm for a 2pm procedure has not been given extra protection - they have been given a longer period of concentrated acid accumulation.
Water is generally permitted up to two to four hours before anaesthesia for most patients. Clear fluid intake does not meaningfully increase gastric volume and may reduce the acidity of gastric contents.
The standard six-hour guideline applies to healthy patients undergoing elective procedures. High-risk patients - those with GI obstruction, delayed gastric emptying, recent vomiting, or large intra-abdominal masses - require individual assessment and may warrant extended fasting, but this should be a considered clinical decision rather than a reflexive extension of the standard protocol.
- Current recommendation is a six-hour fast for food prior to elective anaesthesia in dogs and cats
- Extended fasting beyond six to eight hours does not reduce risk further - it increases gastric acid concentration and volume
- Water can generally be permitted up to two to four hours preoperatively
- High-risk patients require individual fasting assessment, not simply longer standard fasting
Airway management in high-risk patients
In patients with significant reflux risk, airway management decisions are as important as any pharmacological intervention. The key principle is straightforward: minimise the time between loss of consciousness and establishment of a protected airway, and maintain that protection until the patient can reliably protect their own airway.
Rapid induction and intubation. For high-risk patients, the approach should mirror the principles of rapid sequence induction - pre-oxygenation, a prompt and effective induction to an adequate depth, and immediate intubation without delay. The window between induction and intubation is the period of maximum vulnerability. Difficult airway equipment should be immediately available, and the anaesthetist should have a clear plan before induction begins. See the companion module on Cricoid pressure and rapid sequence induction for the full technique.
Cricoid pressure. Cricoid pressure - the application of firm, controlled pressure to the cricoid cartilage to occlude the oesophagus against the vertebral column - is a technique used to reduce passive regurgitation during the vulnerable induction-to-intubation interval. It requires a trained assistant and correct technique to be effective, and must be released immediately upon intubation. Its use should be considered in any patient where the risk of passive regurgitation during induction is judged to be elevated.
Endotracheal tube cuff management. Once the endotracheal tube is placed, appropriate cuff inflation is the critical next step. The cuff creates a physical seal between the pharynx and the trachea - an underinflated cuff provides no meaningful protection against aspiration of pharyngeal material. Cuff pressure should be sufficient to prevent gas leak when tested at a standard airway pressure of 20 cmH₂O.
A low-volume, high-pressure inflation with a small amount of sterile lubricant applied to the cuff surface allows a reliable seal while reducing the risk of mucosal friction injury during placement and tube movement. Cuff pressure should be checked with a manometer rather than estimated by feel - tactile assessment of cuff pressure is notoriously inaccurate.
Low-volume, high-pressure cuff inflation with sterile lubricant applied to the cuff surface gives a reliable seal while minimising mucosal trauma. Always verify the seal at 20 cmH₂O with a manometer - cuff pressure by feel alone is unreliable.
For rapid sequence induction in high-risk patients, have your equipment checked, your dose drawn, and your assistant briefed before induction begins. Once you start, commit to a smooth, swift sequence.
- Minimise the induction-to-intubation interval in high-risk patients - this is the period of maximum vulnerability
- Cricoid pressure reduces passive regurgitation during induction in appropriately selected patients - see companion RSI module for technique
- Cuff inflation should be verified against a standard airway pressure (20 cmH₂O) - not estimated by feel
- Low-volume, high-pressure inflation with sterile lubricant on the cuff provides a reliable seal with reduced mucosal trauma
Proton pump inhibitors and gastric protectants
Pharmacological intervention to reduce gastric acidity is a well-established strategy in high-risk patients. The rationale is straightforward: if reflux cannot be completely prevented, then reducing the acidity of what might be refluxed reduces the severity of the injury if it occurs.
Proton pump inhibitors (PPIs) - omeprazole, esomeprazole, and pantoprazole - irreversibly inhibit the H⁺/K⁺-ATPase pump in gastric parietal cells, substantially reducing acid production. They are more effective and more sustained in action than H₂ antagonists such as famotidine. Oral omeprazole or esomeprazole, administered the evening before and the morning of surgery in dogs, significantly reduces perioperative gastric acidity. Critically, PPIs must be given at least four hours before anaesthesia to allow adequate onset - administering them at induction provides no meaningful benefit. By raising gastric pH, PPIs also indirectly improve LOS tone and reduce the severity of mucosal and pulmonary injury if reflux or aspiration does occur.
It is important to understand what PPIs do and do not do. They reduce the acidity of gastric fluid but they do not reduce gastric volume, and they do not directly prevent reflux. They are one component of a risk-reduction strategy, not a substitute for the rest of it.
Sucralfate can be used in the postoperative period to protect oesophageal and gastric mucosa in patients known to have refluxed or where oesophagitis is suspected. It forms a protective coating over damaged mucosa and promotes healing - it is not a drug for the moment of acute management, but a postoperative tool.
Metoclopramide and other prokinetics increase LOS tone and accelerate gastric emptying. They may be valuable in patients with documented delayed gastric emptying or in high-risk cases where reducing gastric volume at induction is a priority.
- PPIs reduce gastric acidity - by raising pH they also indirectly improve LOS tone and reduce the severity of mucosal and pulmonary injury if reflux or aspiration occurs
- They do not reduce gastric volume or directly prevent reflux - they are one layer of protection, not a complete strategy
- Oral omeprazole or esomeprazole must be given at least four hours before anaesthesia - not at induction
- IV pantoprazole is the option for urgent cases where oral pretreatment has not occurred
- Metoclopramide can reduce gastric volume and improve LOS tone in appropriate patients - avoid in obstruction
- Sucralfate is a postoperative mucosal protectant - use it after the fact, not as prevention
Managing regurgitation when it occurs
Despite best efforts, regurgitation happens. When it does, the speed and quality of the response matters enormously. A calm, structured, stepwise approach gives the patient the best possible chance of a good outcome. Panic, disorganised intervention, or - perhaps most dangerously - failing to recognise that regurgitation has occurred and doing nothing, all worsen outcomes significantly.
The priorities in order are: protect the airway, position for drainage, remove the material, prevent further regurgitation, and plan the recovery carefully.
Securing the airway
Airway security is the foundation of everything else. An endotracheal tube with an appropriately inflated cuff seals the subglottic space and prevents material in the pharynx from entering the trachea - but only if the cuff is correctly placed and adequately inflated.
Cuff pressure should be sufficient to prevent gas leak at a standard airway pressure of 20 cmH₂O, but not so high as to cause tracheal mucosal damage. In the context of regurgitation, err toward adequacy of seal rather than over-caution about mucosal pressure; a brief period of moderate over-inflation is less harmful than tracheal contamination.
If the patient is not intubated when regurgitation occurs - for example, during mask induction or a very short procedure under sedation - intubation must happen as quickly as possible. Use the time available to set up for rapid intubation rather than attempting other manoeuvres first.
Removing regurgitated material
Thorough removal of material from the oral cavity and pharynx is both urgent and technically important. The goal is to clear the entire accessible airway of contaminated material before any of it can be drawn into the trachea.
A wide-bore Yankauer sucker is the correct instrument. The standard narrow-bore suction catheters used for airway suctioning are inadequate for clearing volumes of gastric fluid or any particulate matter. Have one immediately to hand at every anaesthetic - it should be part of the standard setup, not something that needs to be fetched.
Suction should be applied systematically. Start at the back of the oral cavity, suction around the pharynx, and then check the laryngeal area around the endotracheal tube. The area immediately around the cuff is a common site for pooled material to accumulate.
If there is any suspicion that material has entered the trachea despite the cuff being in place, gentle tracheal suctioning through the endotracheal tube can be performed - but avoid prolonged suction runs that risk inducing hypoxia.
Safely recovering and extubating
Recovery from anaesthesia following regurgitation requires heightened vigilance and a more conservative approach to extubation timing. The fundamental question at extubation is whether the patient can reliably protect their own airway: swallowing spontaneously and actively, responsive to stimulation, and showing progressive improvement in conscious level.
Keep the endotracheal tube cuff inflated until the moment of extubation. Extubate with suction ready, and maintain the patient in the head-lowered, neck-extended position - the same position used during the regurgitation event. This encourages any residual pharyngeal material to drain out of the mouth rather than toward the larynx.
Following extubation, continue close monitoring through the early recovery period. Signs that aspiration may have occurred include an unexplained decrease in SpO₂, increased respiratory rate, crackles on auscultation, or coughing. If any of these are present, the patient warrants thoracic radiography.
Never extubate a patient who has regurgitated before they are demonstrating reliable swallowing and airway protective reflexes. An early extubation in a patient with residual pharyngeal contamination is one of the most preventable causes of aspiration pneumonia in the postoperative period.
- Extubation should only occur when the patient is actively swallowing and responsive - not before
- Keep the cuff inflated until the moment of tube removal; deflate and extubate with suction ready
- Maintain the head-lowered, neck-extended position in recovery - the same position used during the event
- Closely monitor SpO₂, respiratory rate, and auscultation in early recovery after any regurgitation event
- A low threshold for thoracic radiography is appropriate when aspiration is suspected
Other management considerations
Managing the aftermath of a regurgitation event extends beyond the anaesthetic period. The oesophagus has been exposed to damaging material; the patient may have aspirated; and the risk of further episodes does not disappear at extubation.
If aspiration is suspected - either because material was visualised at the larynx, SpO₂ dropped during the event, or the patient is showing respiratory signs in recovery - obtain thoracic radiographs as soon as the patient is stable enough. Early radiographic changes may be subtle; a second set 12–24 hours later can be informative if the initial images are equivocal.
The decision to start prophylactic antibiotics in suspected aspiration pneumonia is not straightforward. Gastric contents are not sterile, but aspiration pneumonia in the early stages is often chemical rather than bacterial. Prophylactic antibiotics do not reliably prevent the development of bacterial pneumonia and may select for resistant organisms. In general, antibiotic treatment is reserved for cases where pneumonia has been confirmed radiographically or where clinical deterioration occurs.
Supportive care - oxygen supplementation, careful fluid therapy, close monitoring - is the cornerstone of management in the acute period.
A patient that has refluxed significantly should be assumed to have oesophageal mucosal injury until demonstrated otherwise. Clinical signs in the days following the anaesthetic include hypersalivation, lip-licking, regurgitation of food or water, reluctance to eat, and signs of discomfort around the neck and thorax.
Management focuses on reducing further acid exposure and supporting mucosal healing. A proton pump inhibitor (omeprazole in dogs; famotidine is often better tolerated in cats) should be prescribed for a minimum of three to four weeks. Sucralfate suspension, given before meals, provides a physical protective coating over damaged mucosa. Feeding small, frequent meals of a soft, low-fat diet reduces the acid and bile stimulus.
If clinical signs are severe or fail to resolve, oesophagoscopy is indicated to assess the degree of mucosal injury and rule out stricture formation. Strictures that develop can be managed with balloon dilation, but early identification gives the best outcomes.
Any reflux or regurgitation event should be documented clearly in the anaesthetic record. This includes the time it was observed, the nature and estimated volume of the material, the steps taken in response, and the patient's condition at the end of the procedure.
This documentation ensures continuity of care, allows the attending clinician to inform the owner appropriately, and creates a record that informs future anaesthetic planning. An animal that has refluxed once is at higher risk in subsequent anaesthetics. A clear, factual account written contemporaneously is far more useful - and more defensible - than a vague recollection recorded days later.
A patient with a history of peri-anaesthetic reflux warrants a modified approach for any future anaesthetic. Flag it prominently in the patient record and discuss it at the planning stage rather than on the day.
Considerations include: extended preoperative fasting in patients with known delayed gastric emptying; routine pretreatment with a PPI and potentially a prokinetic; a rapid induction technique with immediate intubation; the lowest effective inhalant concentration through good multimodal analgesia; meticulous attention to patient handling; and a cautious, extended recovery with delayed extubation criteria.
For patients with known chronic reflux, brachycephalic anatomy, or significant underlying GI disease, these modifications should form the standard protocol rather than a reactive adjustment.